
11 April 2026
No Comments
iHuman assignment
iHuman Avery Brook 10 year old slipping grades
Avery Brook
10-year-old
4’7” (140cm)
80.0 lb. (36.4kg)
Reason for Encounter
Slipping Grades
Location
Outpatient clinic with x-ray, ECG, and laboratory capabilities
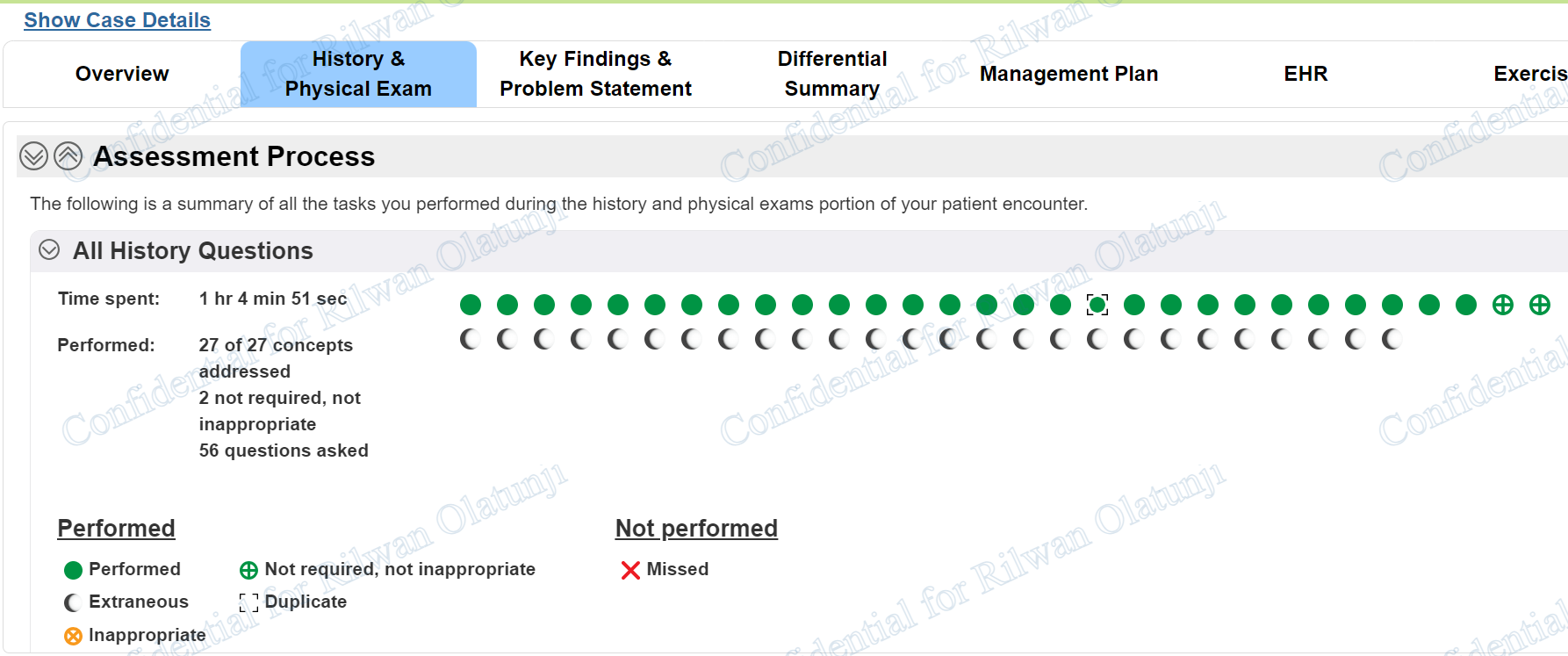
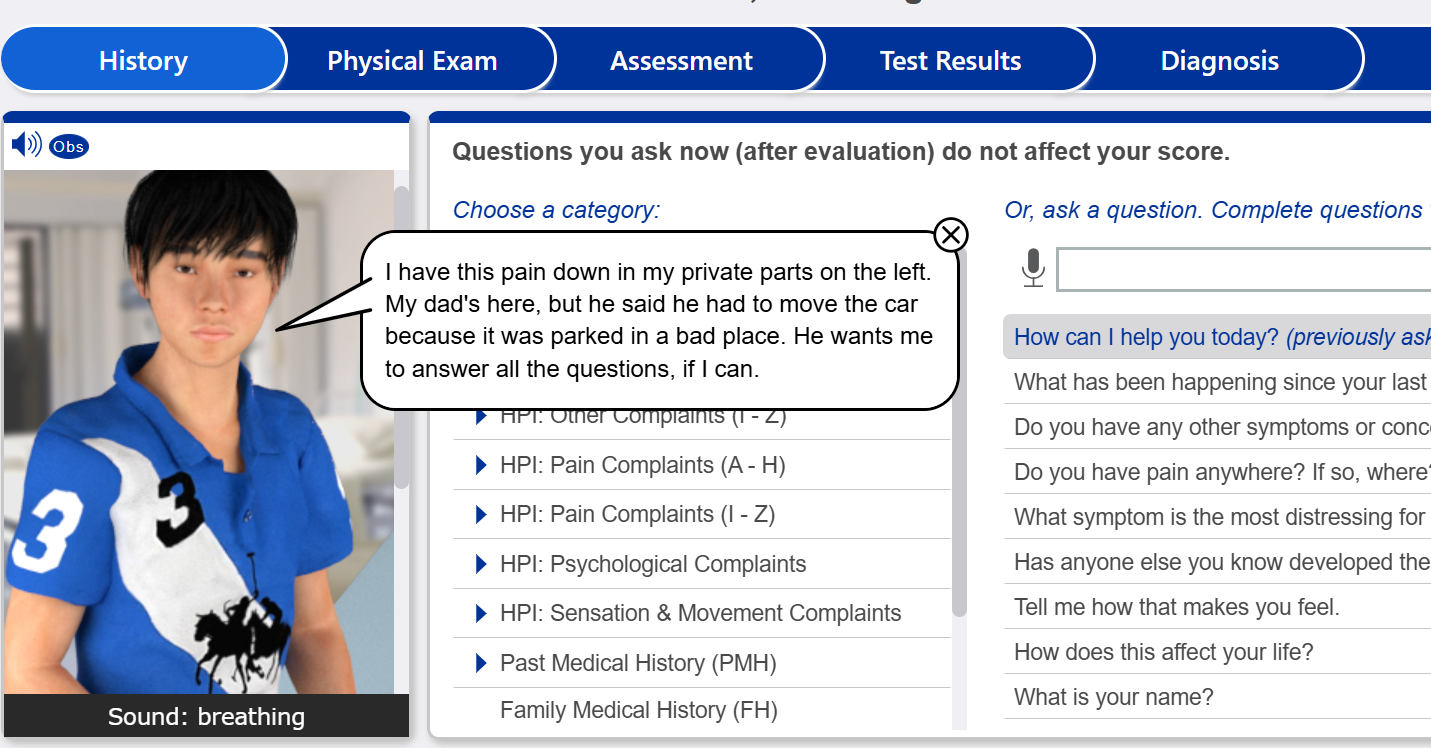
iHuman Avery Brook 10 year old slipping grades History Questions
- How can I help you today? (Patient)
- Do you have any other symptoms or concerns we should discuss? (Patient)
- How can I help her? (Father)
- Does she have any other symptoms or concerns we should discuss? (Father)
- When did her memory problems start? (Father)
- What are the events surrounding the start of her memory problems? (Father)
- Is she having trouble concentrating or making decisions well, if so, how often? (Father)
- When did her trouble concentrating or making decisions start? (Father)
- Are you………
iHuman Avery Brook 10 year old slipping grades
Physical Exams
- Weight
- Height
- cognitive status
- SpO2
- temperature
- blood pressure
- pulse
- respiration
- temperature
- auscultate heart
- auscultate lungs
- assess …….
Case Summary: iHuman Avery Brook Slipping Grades (10-Year-Old)
Navigating complex pediatric neurodevelopmental and behavioral cases in clinical simulation platforms can be a significant academic challenge for nursing and medical students. If you are working through the iHuman simulation for Avery Brook, a 10-year-old female presenting with a primary concern of slipping grades, mastering the clinical workflow from comprehensive subjective history to objective head-to-toe assessment is essential for unlocking the correct diagnostic pathway.
This diagnostic case summary details the critical findings from Avery’s clinical presentation, outlining a systematic workup plan to help you build an accurate differential diagnosis and an effective management plan. For complete interactive walk-throughs, step-by-step guidance, and grading rubrics, explore the comprehensive resources available at the iHuman Tutor Main Website.
Patient Overview & Reason for Encounter
Patient Name: Avery Brook
Age/Developmental Stage: 10-year-old school-aged female
Chief Complaint: Slipping academic performance and grades over a 7-month duration
Students tackling this case must analyze how a seemingly isolated academic issue can stem from complex behavioral, psychological, or physiological origins. Access the full case breakdown and expert-vetted expert tips here: iHuman Avery Brook 10-Year-Old Slipping Grades Answers.
Subjective Workup: Key History Questions Transcript Insights
Unlocking the correct differential diagnosis in this simulation requires a meticulous review of the subjective interview data. Pay close attention to the specific history questions that reveal behavioral patterns across multiple settings:
Chronicity and Timeline: The progressive decline in grades and difficulty focusing began approximately 7 months ago without a distinct environmental trigger.
Pervasiveness of Symptoms: Subjective reports from both her father and her 5th-grade teacher reveal that Avery’s executive challenges are not localized to the classroom. While teachers report excessive classroom talking and frequent lesson interruptions, her father notes pronounced forgetfulness at home, misplacing personal belongings (like shoes), and struggling to finish basic nightly routines.
Behavioral Triggers: Avery explicitly notes that she finds structured schoolwork intensely “boring”. Her father reports situational irritability and verbal arguments that are specifically triggered when transitioning to home evening study sessions.
Crucial Pertinent Negatives: Avery reports feeling “pretty happy all the time” and directly denies experiencing sad thoughts, internalizing anxiety, nervousness, or low mood. Furthermore, there is zero history of peer bullying, sleep disturbances, or recent domestic instability.
Objective Workup: Physical Examination Findings
The physical examination segment of this case is vital for students to rule out organic, structural, or sensory pathologies that could mimic a cognitive or attention deficit.
Vital Signs: Symmetrically stable and normal across all parameters (Temperature: 37.2°C, Pulse: 82 bpm, BP: 102/64 mmHg, RR: 16 bpm, SpO2: 100%).
Sensory Evaluation: Symmetrical visual acuity (20/20 bilaterally via Snellen card) and normal gross hearing. Fundoscopic observation reveals an intact bilateral red reflex and sharp optic disc margins.
Neurological & Coordination Testing: A benign focal neuro assessment demonstrates 5/5 global muscle strength, symmetric 2+ deep tendon reflexes, and completely intact sensory dermatomes. Cerebellar testing—including finger-to-nose and rapid alternating movements—reveals smooth, coordinated, and precise motor execution.
Behavioral & Mental Status Observations: Despite normal neurological function, the objective clinical evaluation is notable for marked physical hyperactivity, constant gross motor fidgeting, inattention to the examiner, and an inability to remain seated or sit still throughout the physical assessment.
Developing the Differential Diagnosis
When synthesizing Avery’s clinical picture, students should formulate a tiered list of differential diagnoses to present during their assessment phase. Consider how the following conditions align with Avery’s history and exam data:
1. Neurodevelopmental Attention and Hyperactivity Disorders
The presence of pervasive inattention, motor impulsivity, excessive talking, and multi-setting functional impairment (home and school) strongly supports an intrinsic executive functioning deficit.
2. Specific Learning Disorders (SLD)
A child struggling with unrecognized reading, writing, or mathematical processing barriers will often experience falling grades and become disengaged or disruptive in class. However, an SLD alone typically does not account for continuous gross motor fidgeting and forgetfulness regarding non-academic chores at home.
3. Pediatric Mood or Anxiety Disorders
Anxiety and childhood depression can manifest atypical symptoms like irritability, concentration difficulties, and academic decline. Avery’s explicit denial of dysphoria, worry, or negative self-thought acts as a key diagnostic indicator to down-rank these differentials.
4. Absence Seizures (Petit Mal)
Staring spells can cause transient lapses in consciousness that mimic classroom inattention and drive down school performance. However, Avery’s primary presentation involves physical restlessness and continuous over-activity rather than sudden, unprovoked pauses in responsiveness.
Developing the Management Plan
To finalize your case simulation successfully, your recommended management plan must incorporate multi-informant behavioral testing and collaborative strategies:
Standardized Rating Scales: Utilize validated diagnostic tools, such as the NICHQ Vanderbilt ADHD Diagnostic Rating Scales (completed independently by both parents and 5th-grade teachers) to objectively quantify symptom frequency and confirm diagnostic criteria.
Academic and Educational Interventions: Coordinate with an educational specialist to evaluate the child for classroom accommodations, such as a 504 Plan or IEP, featuring preferential front-row seating, structured movement breaks, and broken-down task assignments.
Behavioral Therapy: Implement specialized behavioral counseling and parent management training to establish predictable home routines and minimize situational transition friction.