
15 April 2026
No Comments
iHuman assignment
iHuman Brianna Gill Kristina Hart pain when I pee answers NR602
Kristina Hart Brianna Gill
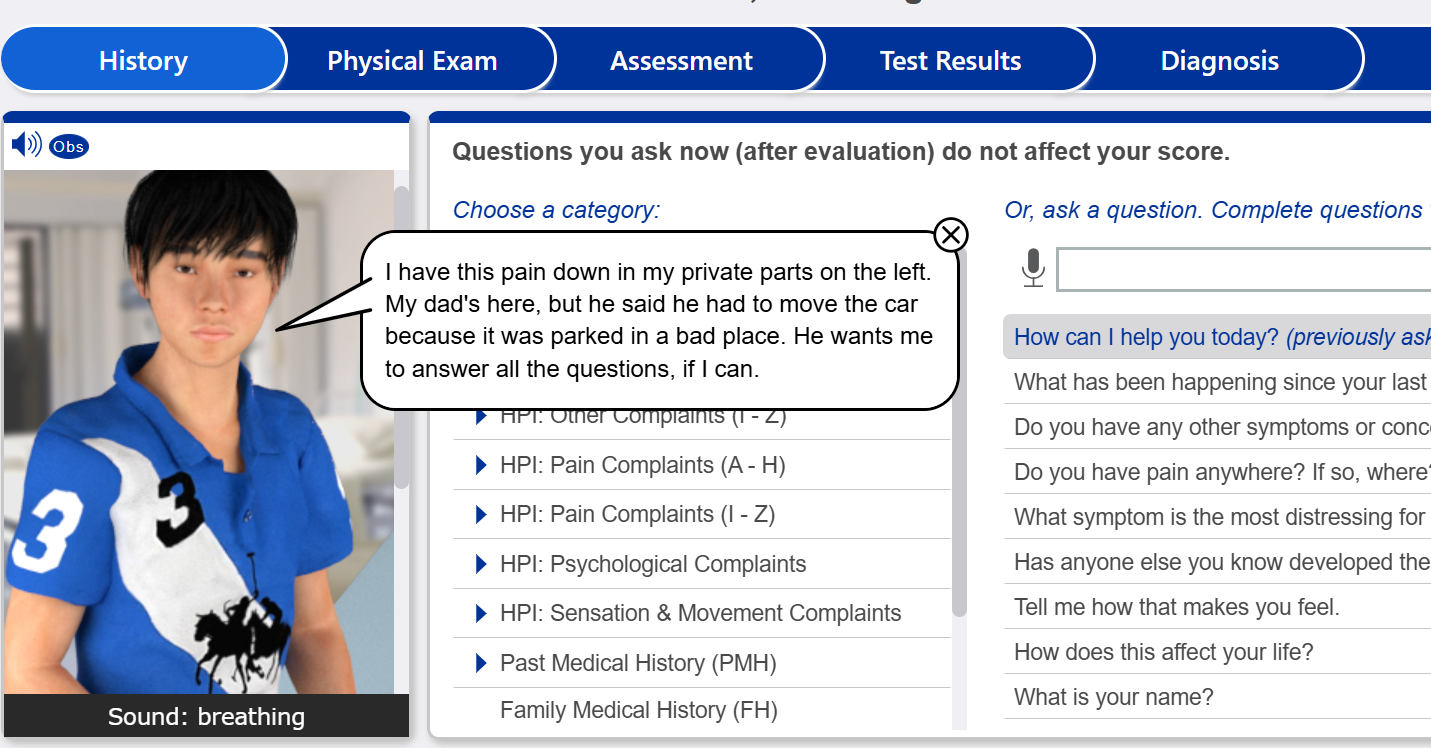
Reason for encounter Pain when I pee
28 y/o
5′ 2″ (157 cm)
132.0 lb. (60.0 kg)
Location
Outpatient clinic with x-ray, ECG, and laboratory capabilities
iHuman Brianna Gill pain when I pee answers NR602
History Questions
- How can I help you today?
- Do you have any other symptoms or concerns we should discuss?
- Do you have pain/discomfort when you urinate?
- When did your pain/discomfort with urination start?
- What are the events surrounding the start of your pain/discomfort with urination?
- Does anything make your pain/discomfort with urination better or worse?
- How severe is your pain/discomfort with urination?
- Does your pain/discomfort with urination come and go?
- Have you passed any stones in your urine?
- How long does your urination pain/discomfort last?
- What treatments have you….
iHuman Brianna Gill Kristina Hart pain when I pee answers NR602
Physical Exams
- Weight
- Height
- cognitive status
- SpO2
- temperature
- blood pressure
- pulse
- respiration
- temperature
- auscultate heart
- auscultate lungs
- assess …….
iHuman Case Study: Brianna Gill / Kristina Hart – Pain When I Pee (28-Year-Old) NR602 Full Case Summary
The iHuman case of Brianna Gill / Kristina Hart, a 28-year-old female presenting with pain when I pee, is a high-yield clinical scenario frequently encountered in the NR602 course. This case emphasizes the importance of distinguishing urinary symptoms from sexually transmitted infections using targeted history questions, physical examination, differential diagnosis, and management plan.
For complete step-by-step iHuman answers, visit:
👉 https://ihumantutor.com/brianna-gill-kristina-hart-pain-when-i-pee-answers-nr602/
Explore all iHuman case solutions here:
👉 https://ihumantutor.com/
Clinical Presentation and History Questions (iHuman Focus)
This 28-year-old patient presents with a primary complaint of pain when I pee, described as a burning sensation with every urination over the past two days. She also reports yellow, thick vaginal discharge, urinary urgency, frequency, and intermittent spotting. These findings are crucial when answering iHuman history questions because they point toward a genitourinary infection beyond a simple urinary tract infection.
Her sexual history significantly elevates risk: she has had multiple partners within the last six months and reports inconsistent condom use, especially during alcohol use. These epidemiologic risk factors strongly support a diagnosis of a sexually transmitted infection (STI). She denies fever, flank pain, nausea, vomiting, or abdominal pain, which helps rule out more severe upper urinary tract involvement.
Understanding how to interpret these iHuman history questions is essential for developing a correct differential diagnosis and management plan.
Physical Examination Findings (iHuman Physical Examination Breakdown)
The physical examination in this iHuman case provides the most critical diagnostic clues. Vital signs are stable, indicating no systemic infection. The abdominal exam shows no tenderness, and there is no costovertebral angle tenderness, reducing suspicion for pyelonephritis.
The pelvic examination is the key diagnostic component. Findings include:
- Mucopurulent discharge in the vaginal canal
- Purulent drainage from the cervical os
- Cervical friability
These findings are classic for cervicitis. Importantly, there is no cervical motion tenderness, which helps rule out pelvic inflammatory disease at this stage.
In many iHuman physical examination scenarios, learners miss the importance of the speculum exam. This case reinforces that pelvic findings are often more diagnostic than urinary symptoms alone.
Differential Diagnosis (NR602 Clinical Reasoning)
The differential diagnosis for pain when urinating in a 28-year-old female includes:
- Cervicitis due to Chlamydia trachomatis
- Gonorrhea infection
- Trichomoniasis
- Urinary tract infection
- Vulvovaginal candidiasis
Among these, cervicitis caused by chlamydia or gonorrhea is the most likely diagnosis due to the combination of discharge, sexual risk factors, and cervical findings.
This case demonstrates a common iHuman trap: assuming all dysuria is a UTI. However, the presence of vaginal discharge and cervical inflammation shifts the diagnosis toward an STI.
Diagnostic Workup (iHuman Management Strategy)
In this iHuman NR602 case, the diagnostic workup should include:
- NAAT testing for chlamydia and gonorrhea (gold standard)
- Vaginal wet mount for trichomoniasis
- Urinalysis to evaluate for concurrent UTI
- Pregnancy test prior to treatment
- HIV and syphilis screening due to high-risk behavior
These tests are essential for confirming the diagnosis and guiding the management plan. Proper selection of diagnostics is often heavily weighted in iHuman grading rubrics.
Management Plan (Evidence-Based iHuman Answers)
The management plan for this case focuses on empiric treatment, symptom control, and prevention of reinfection. According to U.S. guidelines, treatment should cover both chlamydia and gonorrhea.
Recommended therapy includes:
- Ceftriaxone intramuscular injection
- Doxycycline oral therapy for 7 days
This dual therapy approach ensures coverage of the most common pathogens causing cervicitis. In iHuman answers, selecting the correct medications and dosing is critical for full credit.
Supportive care includes NSAIDs such as ibuprofen for pain relief. However, pharmacologic therapy alone is not sufficient without proper patient education.
Patient Education and Prevention Strategies
Patient education is a cornerstone of this iHuman case. The patient should be instructed to:
- Abstain from sexual activity until treatment is complete
- Ensure all sexual partners are tested and treated
- Use condoms consistently to reduce STI risk
- Limit alcohol intake to avoid impaired decision-making
Preventive measures should also include:
- HPV vaccination
- Hepatitis B vaccination
These interventions are essential components of a comprehensive management plan in NR602 and are frequently required in iHuman case submissions.
Follow-Up and Red Flags
Follow-up is recommended within 1–2 weeks if symptoms persist. Retesting at 3 months is essential due to the high risk of reinfection.
Patients must be educated on red flag symptoms, including:
- Fever
- Severe pelvic pain
- Nausea or vomiting
- Worsening discharge
These may indicate progression to pelvic inflammatory disease and require urgent care.
Multimedia Learning Resource
For a deeper understanding of this case and similar iHuman scenarios, watch this detailed video explanation:
🎥 https://youtu.be/Uk08Ynb5cx0?si=l8KtSqzcel-xx613