

3 April 2026
No Comments
iHuman assignment
NR603 i-Human Case Charlie Harris
39 y/o
5′ 8″ (173 cm)
140.0 lb (63.6 kg)
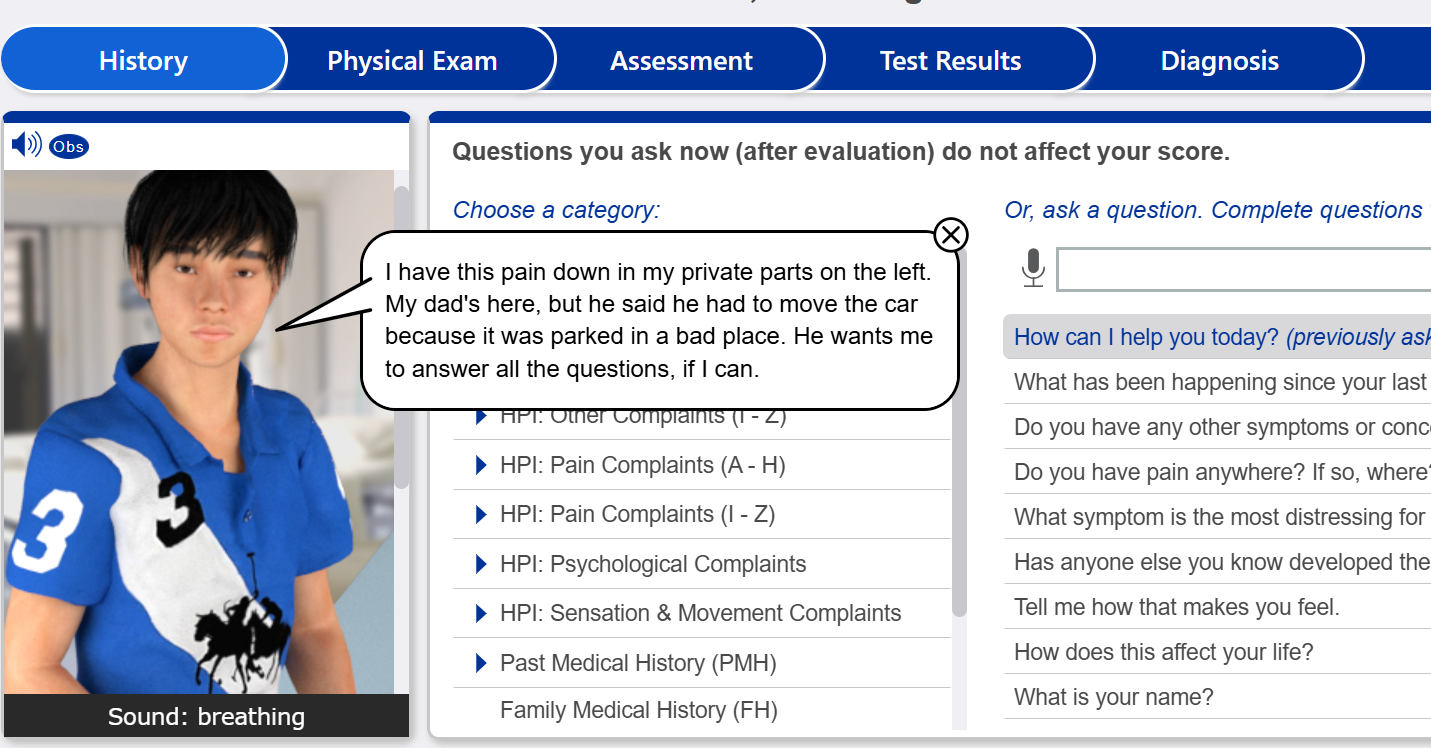
Reason for encounter
Shortness of breath
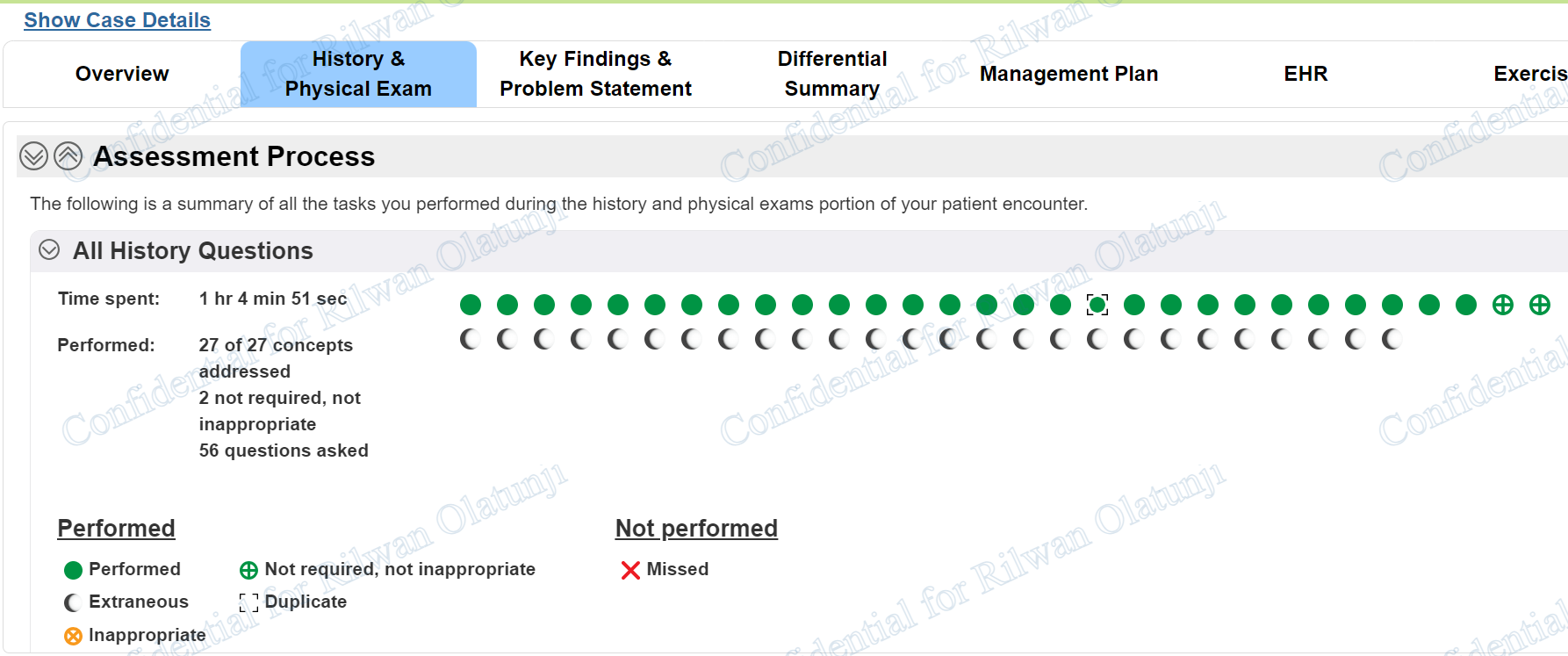
Charlie Harris shortness of breath 39 year old ihuman history questions
- How can I help you today?
- Do you have any other symptoms or concerns we should discuss?
- Have you been having fevers?
- Do you have night sweats?
- Do you wheeze?
- Are you short of breath?
- When did you first notice feeling short of breath?
- How long does your shortness of breath last?
- What are the events surrounding the start of your shortness of breath?
- Does your shortness of breath come and go?
- Does anything make your shortness of breath better or worse?
- Are you short of breath when lying down?
- Are you short of breath at rest?
- How severe is your shortness of breath?
- Do you awaken at night short of breath?
- What treatments have you tried for your shortness of breath?
- Are you………
Charlie Harris shortness of breath 39 year old ihuman physical exams required
- Weight
- Height
- cognitive status
- SpO2
- temperature
- blood pressure
- pulse
- respiration
- temperature
- auscultate heart
- auscultate lungs
- assess …….
iHuman Case Study: Charlie Harris – Shortness of Breath Case Summary
The iHuman case of Charlie Harris presents a classic example of a high-risk patient with progressive shortness of breath requiring careful clinical reasoning. Charlie is a 39-year-old male with a history of untreated HIV who reports a two-week history of worsening dyspnea, dry cough, fever, night sweats, and unintentional weight loss. These key history questions are critical in identifying red flags, especially in immunocompromised patients.
During the physical examination, notable findings include tachypnea (24 breaths per minute), tachycardia, fever (101.2°F), and hypoxia with an SpO₂ of 89%. The patient demonstrates conversational dyspnea and use of accessory muscles, indicating increased work of breathing. Lung percussion remains largely resonant, suggesting a diffuse rather than focal pulmonary process.
Based on the history and exam, the leading differential diagnosis includes Pneumocystis jirovecii pneumonia (PCP), especially given the untreated HIV status. Other considerations include pulmonary tuberculosis and community-acquired pneumonia, though these are less consistent with the nonproductive cough and subacute progression.
The appropriate management plan involves immediate oxygen supplementation, initiation of empiric treatment with trimethoprim-sulfamethoxazole (TMP-SMX), and corticosteroids due to hypoxia. Additional diagnostic workup includes chest imaging, arterial blood gases, and CD4 count.