
10 July 2026
No Comments
iHuman assignment
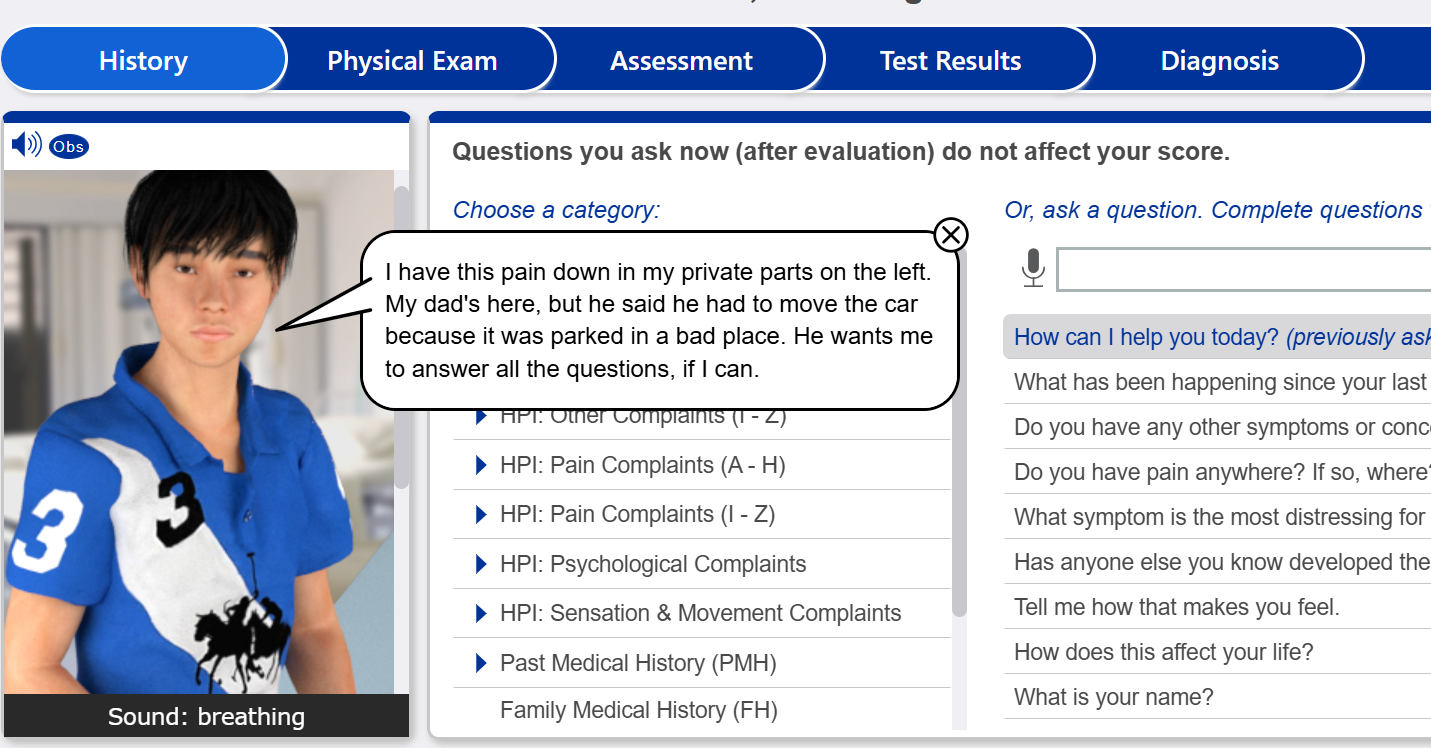
iHuman Sophia King confusion and memory loss 79 year old answers
Sophia King 79 y/o
5′ 4″ (163 cm) 110.0 lb (50.0 kg)
Reason for encounter Confusion and memory loss reported by family member
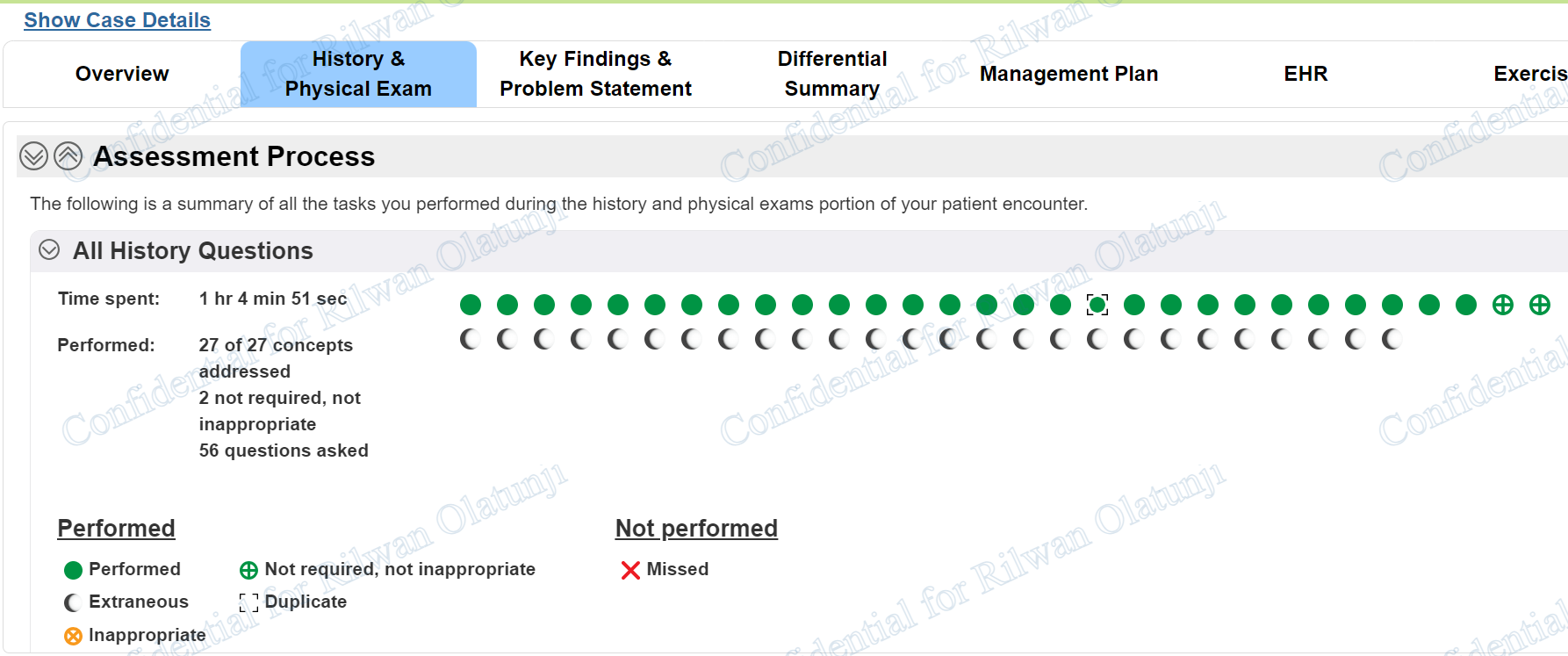
iHuman Sophia King confusion and memory loss 79 year old answers history questions
- How can I help you today?
- Do you have any other symptoms or concerns we should discuss?
- Do you have high blood pressure?
- When did your high blood pressure start?
- Does anything make your high blood pressure better or worse?
- What treatments have you had for your high blood pressure?
- Can you tell me about any current or past medical problems you have had?
- How is your overall health?
- Do you have high cholesterol?
- Do you have heart disease and/or have you ever had a heart attack?
- Are you…..
iHuman Sophia King 79 year old confusion and memory loss answers physical exams required
- Weight
- Height
- cognitive status
- SpO2
- temperature
- blood pressure
- pulse
- respiration
- temperature
- auscultate heart
- auscultate lungs
- assess …….
iHuman Clinical Case Review: Sophia King (79-Year-Old Female with Confusion and Memory Loss)
The diagnostic evaluation of geriatric cognitive decline requires a rigorous, systematic approach to differentiate between primary neurodegenerative disorders and reversible secondary causes. This clinical case review examines the presentation of Sophia King, a 79 year old female presenting with progressive confusion and memory loss.
Designed as a study guide for advanced practice nursing students and medical professionals navigating advanced clinical simulations, this guide covers the core elements of the case—including essential history questions, structured physical examination findings, differential diagnosis strategies, and an evidence-based management plan. For students seeking full interactive walkthroughs, specialized academic assistance can be accessed via iHuman Case Answers and the dedicated iHuman Sophia King Case Study Resource.
Patient Overview & Presenting Clinical Picture
The patient is a 79-year-old retired elementary school teacher who presents to the outpatient clinic accompanied by her daughter. The primary reason for the encounter is an accelerating decline in cognitive performance, short-term recall, and executive functioning over the past six months.
While the patient maintains a high degree of anosognosia—subjectively reporting that she is “doing fine”—her daughter provides crucial collateral history documenting significant functional limitations and behavioral modifications.
Key Subjective History Findings
Onset & Timeline: Subtle memory lapses began approximately one year ago, with marked, rapid progression noted during the last 6 months.
PDFFunctional Decline (IADLs): The patient is no longer safely able to execute complex tasks, including household financial management, meal preparation, and driving. Notable safety indicators include leaving appliances running and getting lost on familiar driving routes.
PDF+ 1Associated Symptoms: Progressive social withdrawal (anhedonia), an unprovoked 8-pound weight loss over a three-month window, and emerging emotional lability characterized by unprovoked irritability and paranoia.
PDFPertinent Past Medical History (PMH): Longstanding hypertension, hyperlipidemia, and coronary artery disease with a history of coronary stent placement. She also has chronic bilateral sensorineural hearing loss managed with hearing aids.
PDF+ 1
For clinicians learning how to structure these initial inquiries, Mastering the correct history questions is critical to establishing a clear chronological timeline of symptoms.
Objective Assessment & Physical Examination
Evaluating a geriatric patient presenting with confusion and memory loss necessitates a combination of a targeted physical assessment and objective neurocognitive screening tools.
Objective Examination Highlights
General Appearance: The patient appears noticeably unkempt and disheveled, exhibiting poor personal hygiene and an odor of stale urine on her clothing.
Neurological & Gait Status: Intact cranial nerves and symmetric deep tendon reflexes; however, her motor assessment reveals a slightly stooped, small-step shuffling gait.
Cardiovascular: Regular rate and rhythm, with the point of maximal impulse (PMI) slightly displaced 2 cm lateral to the midclavicular line. Symmetrical peripheral pulses are intact throughout.
Standardized Neurocognitive Tool Performance:
Mini-Mental State Examination (MMSE): Score of 19/30, signifying moderate cognitive impairment.
Mini-Cog: 1 out of 3 object recall.
Clock-Draw Test: Scored at 4, indicating impaired spatial planning and executive dysfunction.
Geriatric Depression Scale (GDS): 3 out of 15, ruling out severe active pseudodementia secondary to clinical depression.
Differential Diagnosis Framework
When constructing a differential diagnosis for a 79-year-old patient with progressive executive deficit, clinicians must look at both structural neurodegenerative pathologies and potential metabolic, vascular, or infectious mimicries.
A comprehensive clinical workflow considers:
Primary Neurodegenerative Tauopathies / Amyloidopathies: Conditions such as Alzheimer’s disease, particularly when characterized by disproportionate hippocampal and cortical atrophy on structural neuroimaging.
Vascular Dementia: Cognitive impairment secondary to ischemic cerebrovascular events, macrovascular disease, or microvascular white matter changes, strongly correlated with a history of HTN, HLD, and CAD.
Acute-on-Chronic Delirium: Triggered by acute metabolic derangements or silent infections, such as an asymptomatic Urinary Tract Infection (UTI), underscored by new-onset urinary incontinence.
Reversible Reversible Causes of Cognitive Decline: Severe nutritional macrocytic deficiencies (Vitamin B12 or Folate), profound thyroid dysregulation (Hypothyroidism), or chronic infectious encephalopathies (Neurosyphilis/HIV).
Holistic Management Plan & Clinical Interventions
An optimized management plan for advanced cognitive impairment targets both symptom stabilization and comprehensive safety risk reduction.
Pharmacological Strategy
Cholinesterase Inhibitors: Initiating agents such as donepezil to optimize cholinergic neurotransmission, typically titrated carefully to manage potential gastrointestinal side effects and monitor weight stability.
NMDA Receptor Antagonists: Incorporating memantine (Namenda) concurrently for dual-pathway neuroprotection in moderate-to-severe cognitive presentations.
Medication De-escalation: Critical evaluation of sedating or anticholinergic drugs—such as PRN zolpidem—which increase the risk of nocturnal confusion and falls.
Supportive & Interdisciplinary Care
Safety & Mobility Interventions: Formal physical and occupational therapy evaluations to optimize home safety, implement fall prevention strategies (removing loose rugs, installing grab bars), and manage driving cessation.
Caregiver Support & Legal Coordination: Social work referrals to facilitate discussions regarding long-term memory care options, community resource alignment, and advance care planning (living wills and durable power of attorney).
Optimize Your Clinical Simulation Performance
Synthesizing complex subjective and objective findings is a foundational skill for advanced nursing practice. Navigating diagnostic reasoning within digital platforms requires a strong grasp of geriatric care principles and diagnostic workflows.
To explore similar case structures, clinical problem statements, and detailed interactive simulations, visit iHuman Tutor for comprehensive academic support. For specific review materials on this study, reference the complete iHuman Sophia King Case Solutions Guide to enhance your clinical synthesis skills.